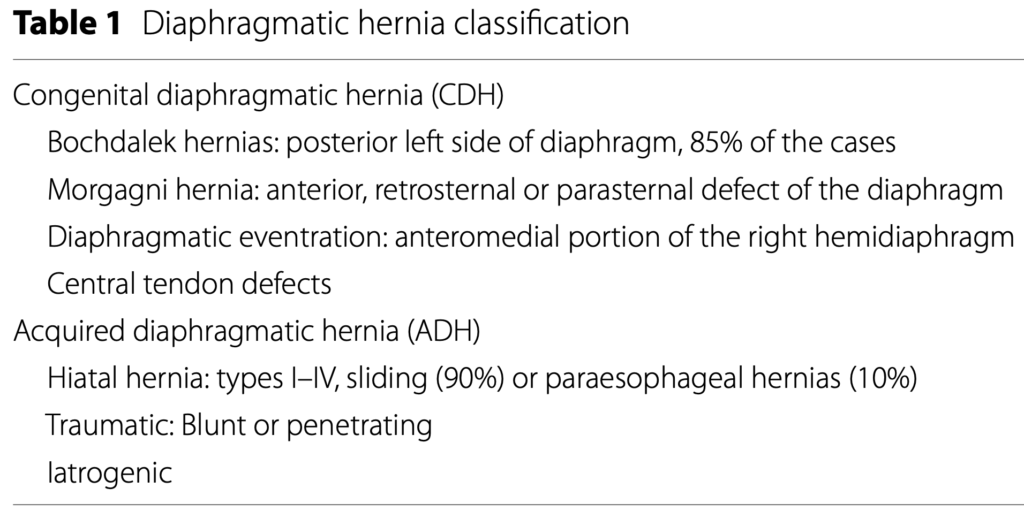
Introduction
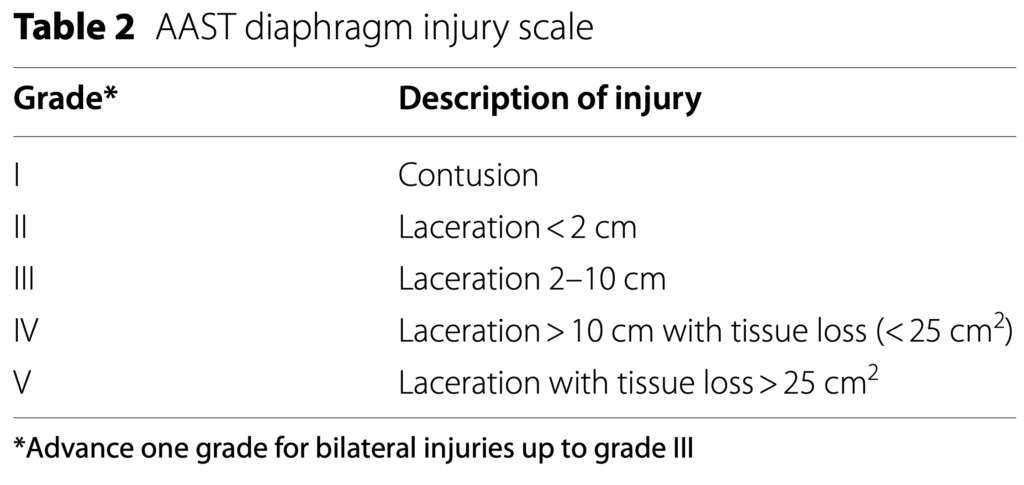
Diaphragmatic rupture occurs in 2.1% of blunt trauma and 3.5% of penetrating trauma. Overall, diaphragmatic rupture (DR) is infrequent and may reach up to 5% of trauma patients depending on the injury severity and mechanism of injury.
The distribution of diaphragmatic hernia after blunt trauma is as follows: 50–80% affect the left hemidiaphragm, 12–40% affect the right side, while 1–9% are bilateral.
What is the best way to diagnose DH in the emergency setting?
In patients without a history of trauma and with respiratory symptoms, a chest X-ray both anteroposterior and lateral is recommended as the first diagnostic study.
(Strong recommendation based on low-quality evidence, 1C).
In stable trauma patients with suspected DH (non-specific symptoms and chest X-ray), CT scan with contrast enhancement of the chest and abdomen is recommended.
(Strong recommendation based on moderate-quality evidence, 1B).
In stable trauma patients with lower chest penetrating wounds and suspected DH (nonspecific symptoms and chest X-ray), diagnostic laparoscopy is recommended.
(Weak recommendation based on low-quality evidence, 1C).
Endoscopy is not recommended in traumatic hernias.
(Weak recommendation based on low-quality evidence, 2C).
In pregnant patients with suspected non-traumatic DH, ultrasonography is suggested as the first diagnostic study
(Weak recommendation based on very low-quality evidence, 2D).
In stable pregnant patients with suspected non-traumatic DH, MRI is suggested after ultrasonography.
(Weak recommendation based on very low-quality evidence, 2D).
Explanations
However, initial radiographic findings can be misinterpreted in around 25% of the cases.
CT scan is the gold standard for diagnosing the diaphragmatic hernia. It has a sensitivity and specificity of 14–82% and 87%, respectively. Nevertheless, it may miss small tears of penetrating injuries like stab wounds, when no hernia has yet occurred.
What is the best treatment for patients with traumatic diaphragmatic hernia?
Surgery is recommended in stable patients with traumatic DH, preferably with a laparoscopic approach
(Strong recommendation based on moderate-quality evidence, 1B)
In unstable TDH patients, a laparotomy approach is suggested
(Weak recommendation based on low-quality evidence, 2C)
Technical issues
Sac excision is not suggested
(Weak recommendation based on very low-quality evidence, 2D)
Defect repair using non-absorbable sutures is suggested
(Weak recommendation based on low-quality evidence, 2C)
Mesh use is suggested for defects that cannot be closed with direct suture
(Weak recommendation based on low-quality evidence, 2C)
Biosynthetic, biologic or composite meshes are suggested due to the lower rate of hernia recurrence, higher resistance to infections and lower risk of displacement*
(Weak recommendation based on low- quality evidence, 2C)
Percutaneous endoscopic gastrostomy (PEG), gastrostomy or jejunostomy are suggested in patients with oral intake difficulties
(Weak recommendation based on low-quality evidence, 2C)
Preemptive anti-reflux surgery is not suggested in the emergency traumatic DH setting or complicated hernia
(Weak recommendation based on very low-quality evidence, 2D)
Damage Control Surgery (DCS) is recommended in case of patients with intraoperative instability, hypothermia, coagulopathy, significant acidosis or impossibility to close the diaphragm
(Strong recommendation based on low-quality evidence, 1B)
Explanation
Several studies (meta-analysis, reviews and case series) propose primary repair for the diaphragmatic defects with non-absorbable sutures. This should always be attempted when possible. This is classically done in two layers using interrupted non-absorbable mattress suture. Majority of surgeons still prefer using interrupted non-absorbable 2–0 or 1–0 monofilament or braided sutures in two layers.
Suturing defects has the benefit of providing a flat surface for placement of the mesh, preventing mesh extrusion through the defect. In a DH with larger defects (>3 cm), an attempt to primary repair the defect could lead to excessive tension due to the considerable loss of tissue. A very high recurrence rate of 42% has been reported after primary DH repair. In order to reinforce the suture repair, a mesh should be used.
It was recommended not to perform primary closure of the diaphragm if the distance between the edge of the remaining part of the diaphragm and the chest wall is more than 3–4 cm. Primary diaphragmatic suture or mesh reconstruction can seal the chest cavity without paradoxical chest movement or increase in mortality. Many different materials can be used for the reconstruction, mostly favored by the surgeon’s experience, attitude and preference. The reconstruction is typically performed with synthetic meshes. They are well tolerated, can be bio-prosthetic materials or entirely artificial mesh, either absorbable or non-absorbable. Many reviews have evaluated the role of different meshes in DH repair. A mesh should be used for larger defects. Biological meshes have lower rate of hernia recurrence, higher resistance to infections and lower risk of displacement compared with synthetic meshes. An alternative to biological meshes for the repair, particularly of the clean-contaminated and contaminated diaphragmatic hernia repair, is an absorbable synthetic mesh. Absorbable synthetic mesh has the prospective advantages of reduced cost and minimal constraints in manufacturing alternative sizes. Because of
its strength and impermeability, polytetrafluoroethylene (PTFE Gore-Tex) is one of the most common meshes recommended for diaphragmatic reconstruction. It has an advantage of not adhering to the bowel with reduced risk of bowel fistulation. Despite several advantages of using absorbable synthetic mesh, data on diaphragmatic hernia repair in the emergency setting are not available and further studies are warranted.
What is the best treatment for patients with non‐traumatic diaphragmatic hernia?
Surgery is recommended in complicated non-traumatic DH
(Strong recommendation based on moderate-quality evidence, 2C)
In unstable non-traumatic complicated DH patients, a laparotomy approach is suggested
(Weak recommendation based on low-quality evidence, 2C)
In stable patients with complicated non-traumatic DH, minimally invasive approach is suggested
(Weak recommendation based on very low-quality evidence, 2D)
Sac excision is not suggested
(Weak recommendation based on very low-quality evidence, 2D)
Defect repair using non-absorbable sutures is suggested
(Weak recommendation based on low-quality evidence, 2C)
Mesh use is suggested especially for larger defects that cannot be closed
(Weak recommendation based on low-quality evidence, 2C)
Biosynthetic, biologic or composite meshes are suggested due to the lower hernia recurrence, higher resistance to infections and lower risk of displacement.
(Weak recommendation based on low-quality evidence, 2C)
Gastropexy is suggested in patients with gastric volvulus in order to prevent recurrence
(Weak recommendation based on moderate-quality evidence, 2B)
Percutaneous endoscopic gastrostomy (PEG), gastrostomy or jejunostomy are suggested in patients with preexisting oral intake difficulties
(Weak recommendation based on low-quality evidence, 2C)
Gastrostomy and PEG are suggested to provide fixation of the anterior stomach to the abdominal wall in patients unsuitable or high-risk candidates for a definitive surgical procedure, only in case of non-ischemic stomach
(Weak recommendation based on low-quality evidence, 2C)
Anti-reflux surgery is recommended especially in congenital diaphragmatic hernia repair and in patients with gastroesophageal reflux
(Weak recommendation based on low-quality evidence, 2C)
Toupet or Nissen fundoplication is suggested in case of gastroesophageal disease.
(Weak recommendation based on low-quality evidence, 2C)
Thoracoscopy combined with laparoscopy is suggested especially in complicated DH with history of chronic herniation in order to reduce visceral-pleural adhesions and to avoid intrathoracic visceral perforation
(Weak recommendation based on very low- quality evidence, 2D)
Explanations
Several papers advice that the mesh overlaps the defect edge by 1.5–2.5 cm. When tension-free primary closures are difficult, for defects larger than 8 cm or an area of more than 20 cm2, the interposition of a graft can be used successfully. Mesh can be fixed using tackers or transfascial sutures. Tackers should be avoided in proximity of the pericardium because of the risk or cardiac complications.