Reza L, Gottgens K, Kleijnen J, Breukink S, Ambe PC, Aigner F, et al. European Society of Coloproctology: Guidelines for diagnosis and treatment of cryptoglandular anal fistula. Color Dis 2023:1–52. doi:10.1111/codi.16741.
Diagnosis, classification and preoperative investigations
Immediate fistulotomy at incision and drainage of an acute peri-anal abscess is not recommended.
Low-level evidence. [Upgraded by the Guideline Development Group (GDG), expert opinion]
Following incision and drainage of an acute perianal abscess, routine packing should not be practiced.
Low-level evidence. [Upgraded by GDG, expert opinion]
Following incision and drainage of an acute perianal abscess, an empiric course of antibiotics is not recommended to prevent fistula development.
Low-level evidence. [Upgraded by GDG, expert opinion]
A course of antibiotics can be considered following incision and drainage of an acute perianal abscess in patients with systemic sepsis and immunocompromised status.
[GDG expert opinion]
Clinical assessment in patients with an anal fistula must include history and clinical examination to assess for other causes of fistula formation.
[Upgraded by GDG, expert opinion]
Modifiable risk factors for poor wound healing, such as smoking, diabetes and obesity, should be assessed and discussed with patients with an anal fistula prior to attempting reparative surgery.
[Upgraded by GDG, expert opinion]
Investigations to exclude Crohn’s disease should be performed in patients with an anal fistula if there is a clinical history in keeping with inflammatory bowel disease or examination that reveals features suspicious for Crohn’s disease*.
[Upgraded by GDG, expert opinion]
Use of anal manometry is not currently recommended in routine clinical practice in patients with an anal fistula.
[GDG expert opinion]
Examination under anaesthesia (EUA) alone should not be used as a diagnostic tool in complex fistula as MRI and endoanal ultrasound (EAUS) are superior.
Moderate-level evidence.
Imaging by either MRI or EAUS should be utilized with a very low threshold in patients, to differentiate patients with simple from those with complex fistulas.
[Upgraded by GDG, expert opinion]
Preoperative MRI should be used for anal fistula suspected to be complex on clinical assessment, or when EAUS evaluation is not sufficient to assess complexity or is not available.
Moderate level evidence.
Preoperative EAUS can be considered as a primary tool to assess most patients affected by anal fistula, or where MRI is not readily available or there is a need to assess specific clinical features.
[GDG expert opinion]
1.2 Perioperative care
No recommendation can be made for the use of preoperative antibiotics in patients with anal fistula.
[GDG expert opinion]
No recommendation can be made for the use of preoperative bowel preparation in patients with anal fistula.
[GDG expert opinion]
Sitz bath can be considered according to surgeon or patient preference postoperatively in anal fistula.
[GDG expert opinion]
1.3 Partial sphincter-preserving procedures
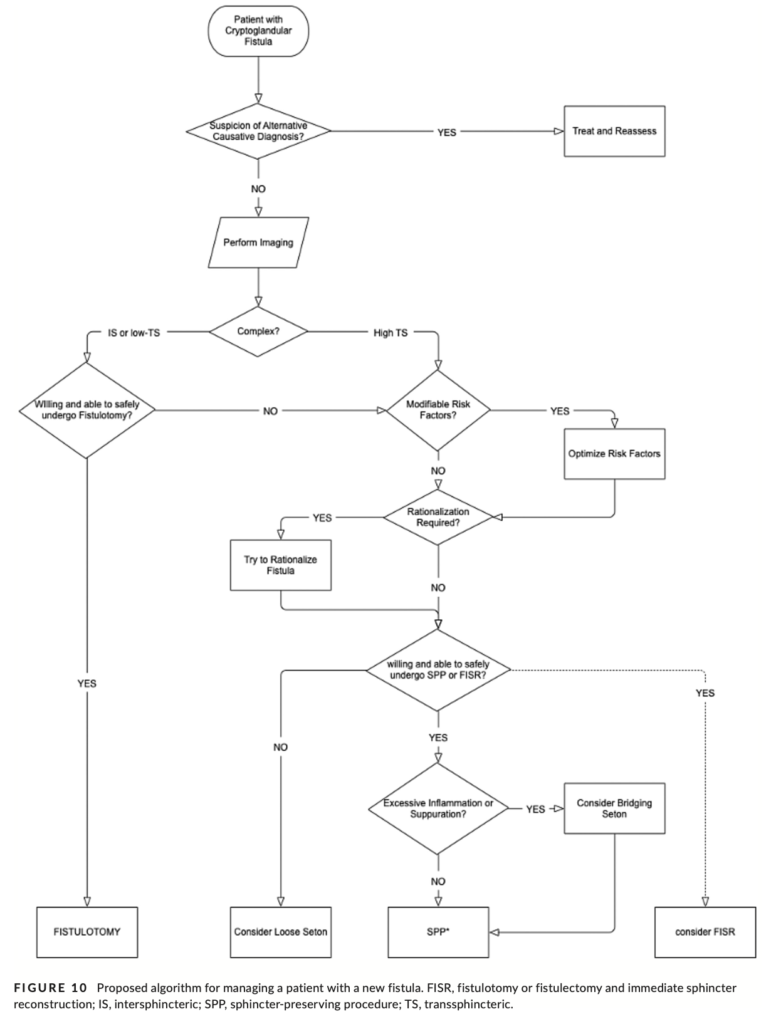
Fistulotomy should be used in patients with intersphincteric or low transsphincteric anal fistula and normal preoperative con- tinence, following a thorough assessment of fistula anatomy, symptomatology, involvement of sphincters, risk of incontinence and exploration of patient expectations.
Moderate-level evidence. [Upgraded by GDG, expert opinion]
Fistulotomy or fistulectomy and immediate sphincter reconstruction (FISR) could be used in highly selected patients with high transsphincteric anal fistula.
Low-level evidence.
Marsupialization could be performed following fistulotomy and fistulectomy for simple anal fistula.
Low-level evidence.
Cutting seton should not be used in the management of simple anal fistula.
Low-level evidence. [Upgraded by GDG, expert opinion]
Cutting seton is not recommended in high anal fistula.
Low-level evidence. [Upgraded by GDG, expert opinion]
Loose setons can be considered as a long-term solution in patients who have complex, recurrent fistulas and are at risk of worsening incontinence from further invasive treatment.
Very low-level evidence. [GDG expert opinion]
Loose setons can be considered as a long-term solution in patients who do not want to have further surgery.
Very low-level evidence. [GDG expert opinion]
Bridging setons can be considered in patients prior to any sphincter-preserving procedure in the presence of excessive inflammation and suppuration, or for whom poor healing is a concern.
Very low-level evidence. [GDG expert opinion]
1.4 Sphincter-preserving procedures
Advancement flap should be used for the management of high anal fistula.
Low-level evidence. [Upgraded by GDG, expert opinion]
There is insufficient data to recommend either core-out or curettage as superior when used with rectal advancement flap. Either method could be selected.
[GDG expert opinion]
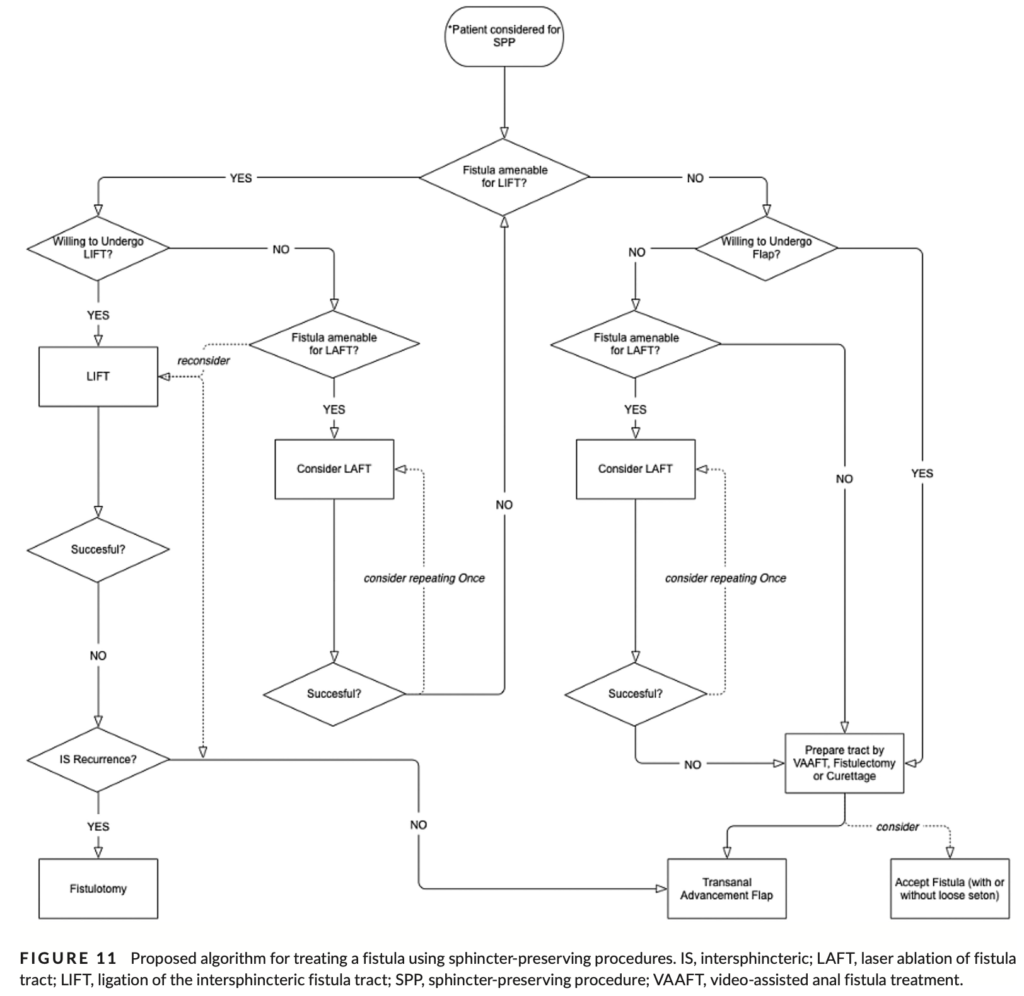
Ligation of the interspincteric fistula tract (LIFT) should be used in the primary treatment of new, high, transsphincteric anal fistulas.
Low-level evidence. [Upgraded by GDG, expert opinion]
No recommendation can be made for the use of BioLIFT because of the lack of high-level evidence for efficacy and long-term outcomes.
Very low-level evidence. [GDG expert opinion]
Video-assisted anal fistula treatment (VAAFT) can be considered in the management of complex perianal fistula.
Very low-level evidence.
Laser ablation of fistula tract (LAFT) can be considered in patients with a high anal fistula.
Very low-level evidence.
Repeated LAFT can be considered in patients following failure from the first attempt. However, repeat procedures should be un- dertaken with caution, as the cumulative effect of LAFT on the sphincter complex is unknown.
Very low-level evidence. [GDG expert opinion]
Fistula plug can be considered in the management of anal fistula.
Low-level evidence. [Downgraded by GDG, expert opinion]
No recommendation can be made for the use of over-the-scope clip (OTSC) in the management of anal fistula.
Very low-level evidence. [GDG expert opinion]
No recommendation can be made for the use of anocutaneous flap in the management of anal fistula.
Very low-level evidence. [GDG expert opinion]
Fibrin glue should not be used in the management of anal fistula.
Moderate-level evidence.
No recommendations can be made for the use of platelet rich plasma (PRP) alone in the management of anal fistula.
Very low-level evidence. [GDG expert opinion]
PRP can be considered in the management of anal fistula as an add-on treatment to LIFT.
Very low-level evidence [Downgraded by GDG, expert opinion]
No recommendation can be made for the use of collagen matrix in the management of anal fistula.
Very low-level evidence. [GDG expert opinion]
No recommendation can be made for the use of suture repair of the internal opening alone in the management of anal fistula.
[GDG expert opinion]
No recommendation can be made for the use of rerouting in high anal fistulas because of a lack of robust data.
[GDG expert opinion]
1.5 Special considerations
A palliative seton can be considered for the management of recurrent perianal sepsis.
[GDG expert opinion]
Palliative seton can be offered to patients with an anal fistula who are keen to avoid further surgical intervention and a risk of injury to the sphincter mechanism.
[GDG expert opinion]
A defunctioning stoma can be considered in patients with severe and locally uncontrollable perianal sepsis with an anal fistula.
[GDG expert opinion]
Details
This means that at least 50% of fistulas present at the time of primary abscess drainage will resolve spontaneously.
Fixed effects analysis of available data at the 1-year follow-up demonstrated a threefold increase in incontinence rate following immediate fistula treatment compared with incision and drainage alone.
On the basis that half of patients will not present with a persistent fistula and given that the risks of false passage and continence impairment only occur with probing and lay open of fistula, although the risk of ‘recurrence’ is lower after immediate fistulotomy, the overall benefit of this intervention is hard to define, and the increased risks associated with it are hard to justify, given the evidence presented in these RCTs. The GDG does not advocate immediate fistula treatment at primary abscess drainage.
The GDG agreed that there is no significant evidence demonstrating that antibiotic treatment following incision and drainage of perianal abscess prevents fistula development; moreover, as injudicious use of antibiotics may contribute to antibiotic resistance, antibiotics should not be used routinely in such patients.
Following a perianal abscess in cryptoglandular disease, 15% of patients will present with a persistent fistula tract.
Hospital Episodes Statistics data from the UK indicate that 3% of patients presenting with a primary perianal abscess will be diagnosed with Crohn’s disease a median of 14 months later.
‘Simple’ anal fistulas include subcutaneous, intersphincteric or low transsphincteric fistulas with minimal involvement of the sphincter complex. ‘Complex’ anal fistulas are extrasphincteric, suprasphincteric or high transsphincteric fistulas involving greater than 30% of the external anal sphincter (EAS) and intersphincteric fistulas involving greater than 50% of the IAS. Rectovaginal fistula, anterior fistula in women, recurrent fistula and fistulas with horseshoe or multiple extensions are also classified as complex fistulas.
In simple anal fistula, the weighted average fistula healing rate for sphincter-cutting procedures was 93.7% (range: 61%–100%) and for sphincter-preserving procedures (LIFT, glue, Permacol paste, OTSC, laser treatment) was 77.7% (range: 25%–100%).
Minor and major incontinence was recorded in 12.7% of patients (and major incontinence alone in 6% of patients) following treatment with sphincter-cutting procedures.
Iqbal et al. conducted pooled analysis of fistula healing in 21 studies and reported a primary fistula healing rate of 93% (95% Cl: 91%–95%, I2 = 51%, p < 0.004) after FISR. Ratto et al. reported a similar success rate for primary fistula healing, with a weighted average healing rate of 93.2% (range: 85.7–100), at a follow-up of 28.9 (range: 12–81) months. Ratto et al. reported a weighted average time to recurrence of 8.9 (range: 1.5–20) months.
The three main types of advancement flap are mucosal, partial or full thickness. Full-thickness flaps involve the entire IAS. The fistula tract is managed either with curettage or with core-out fistulectomy.
Stellingwerf et al. reported an overall rate of fistula healing, following the use of advancement flap in high cryptoglandular anal fistula, of 74.6% (95% CI: 65.6–83.7).
Subgroup analysis found that the lowest recurrence rate occurred for FTAF (7.4%, 95% CI: 4%–10%), followed by PTAF (22.9%, 95% CI: 15.6%– 30.2%) and then MTAF (26.7%, 95% CI: 13.7%–39.7%). Balciscueta et al. also found no marked difference in the recurrence rate between curettage (18.9%, 95% CI: 14.9%–23%) and core-out fistulectomy (21%, 95% CI: 14.9%–25.5%) [97]. Balciscueta et al. included one RCT in which partial-thickness and mucosal advancement flaps were compared; it was found that PTAFs resulted in a significantly higher overall healing rate than MTAFs (90% vs. 60%, p < 0.05).
The weighted incontinence rate reported by Stellingwerf et al., of nine studies, was 7.8% (95% Cl: 3.3%–12.4%, I2 = 56.7%).
Pooled analysis of the incontinence rate following MTAF was 9.3% (95% CI: 5.4%–13.1%, I2 = 39.4%; p = 0.17), for PTAF it was 10.2% (95% CI: 0.5%–14.6%, I2 = 0%; p = 1.0) and for FTAF it was 20.4% (95% CI: 14.2%–26.6%, I2 = 44.5%; p = 0.17). Subgroup analysis found that the incontinence rate following core-out fistulectomy was 14.3% (95% CI: 7.2%–21.3%, I2 = 78.83%; p < 0.001) and following curettage it was 12% (95% CI: 4%–19.2%, I2 = 49.5%; p = 0.1) [97]. There were no significant differences in recurrence rates and incontinence between core-out and curettage of the fistula tract. Mean follow up was 30.3 months (95% CI: 29–31.6) months.
sphincteric anal fistula. The fistula tract should cross the inter- sphincteric space relatively directly and not travel within it. There should be no intersphincteric complexity (such as branching or horseshoeing), the intersphincteric space must be appreciable and the IAS should be intact, meaning a small internal opening without IAS loss. There should also be adequate space cephalad to the fistula to dissect around the fistula completely without risk to rectal wall or vagina, making some very high tracts unsuitable for LIFT.
There were only two RCTs of LIFT. Pooled weighted analysis found a success rate, for LIFT, of 69.1% (95% CI: 53.9%–84.3%). There was high heterogeneity between studies, of I2 = 91.3%.
Stellingwerf et al. reported an incontinence rate of 1.6% (95% Cl: 0.4%–2.8%) in patients following LIFT. This is similar to the rate reported in the meta-analysis published by Emile et al., namely that incontinence of a minor grade was 1.4%. The weighted mean rate of faecal incontinence was 0.6%
In the LIFT group, the fistula healing rate was 85% compared with 79.5% in the advancement flap group. There was no significant difference in postoperative incontinence.
Platelet rich plasma is obtained using centrifugation to concentrate a patient’s own plasma, thus increasing the numbers of platelets and growth factors. It has been used in complex anal fistula, often as an adjunct to other sphincter-preserving procedures, such as LIFT and mucosal advancement flap.