Di Saverio S, Podda M, De Simone B, Ceresoli M, Augustin G, Gori A, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. World Journal of Emergency Surgery; 2020;15:27. https://wjes.biomedcentral.com/articles/10.1186/s13017-020-00306-3
Diagnosis
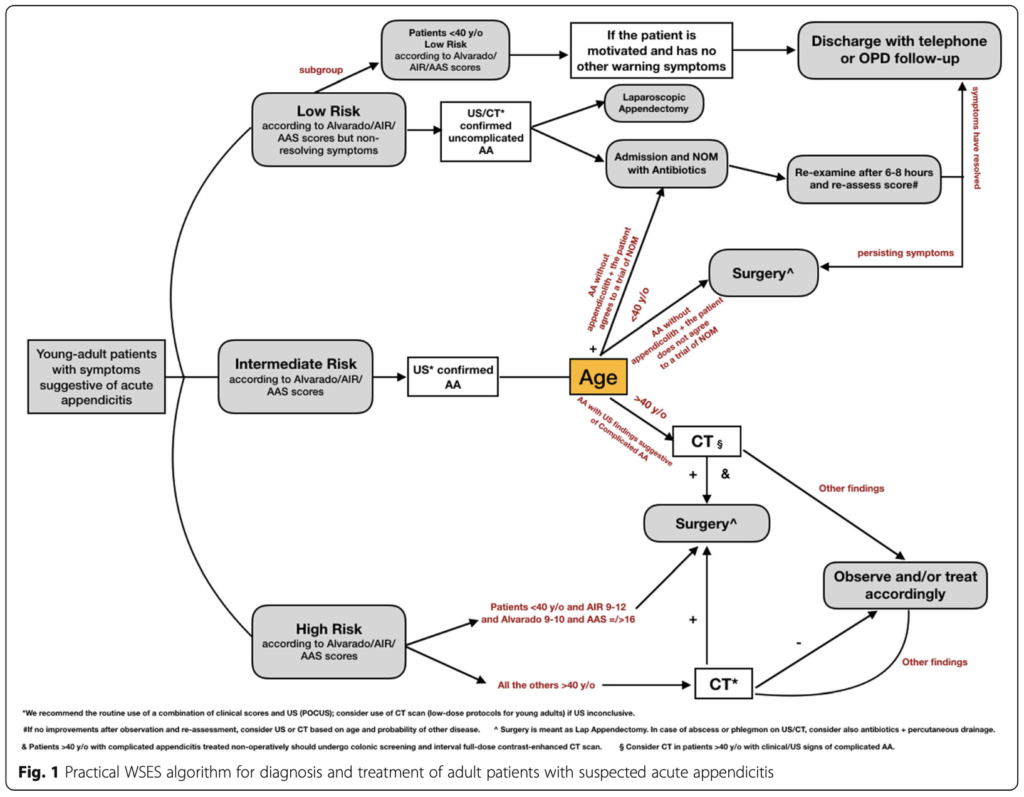
Recommendation 1.1 We recommend to adopt a tailored individualized diagnostic approach for stratifying the risk and disease probability and planning an appropriate stepwise diagnostic pathway in patients with suspected acute appendicitis, depending on age, sex and clinical signs and symptoms of the patient
[QoE: Moderate; Strength of recommendation: Strong; 1B].
Recommendation 1.2.1 We recommend the use of clinical scores to exclude acute appendicitis and identify intermediate-risk patients needing of imaging diagnostics
[QoE: High; Strength of recommendation: Strong; 1A].
Recommendation 1.2.2 We suggest not making the diagnosis of acute appendicitis in pregnant patients on symptoms and signs only. Laboratory tests and inflammatory serum parameters should always be requested
[QoE: Very Low; Strength of recommendation: Weak; 2C].
Recommendation 1.3 We suggest against the use of Alvarado score to positively confirm the clinical suspicion of acute appendicitis in adults
[QoE: Moderate; Strength of recommendation: Weak; 2B].
Recommendation 1.4 We recommend the use of AIR score and AAS score as clinical predictors of acute appendicitis
[QoE: High; Strength of recommendation: Strong; 1A].
Recommendation 1.5 In pediatric patients with suspected acute appendicitis, we suggest against making a diagnosis based on clinical scores alone
[QoE: Low; Strength of recommendation: Weak: 2C].
Recommendation 1.6.1 In evaluating children with suspected appendicitis, we recommend to request routinely laboratory tests and serum inflammatory biomarkers
[QoE: Very Low; Strength of recommendation: Strong: 1D].
Recommendation 1.6.2 In pediatric patients with suspected acute appendicitis, patients.
we suggest adopting both biomarker tests and scores in order to predict the severity of the inflammation and the need for imaging investigation
[QoE: Very Low; Strength of recommendation: Weak: 2D].
Recommendation 1.7 We recommend the routine use of a combination of clinical parameters and US to improve diagnostic sensitivity and specificity and reduce the need for CT scan in the diagnosis of acute appendicitis. The use of imaging diagnostics is recommended in patients with suspected appendicitis after an initial assessment and risk stratification using clinical scores
[QoE: Moderate; Strength of recommendation: Strong; 1B].
Recommendation 1.8 We suggest proceeding with timely and systematic diagnostic imaging in patients with intermediate-risk of acute appendicitis
[QoE: Moderate; Strength of recommendation: Weak; 2B].
Recommendation 1.9 We suggest that cross-sectional imaging (i.e., CT scan) in high-risk patients younger than 40 years old (with AIR score 9–12 and Alvarado score 9–10 and AAS ≥ 16) may be avoided before proceeding to diagnostic +/− therapeutic laparoscopy
[QoE: Moderate; Strength of recommendation: Weak; 2B]
Recommendation 1.10 We recommend POCUS as the most appropriate first-line diagnostic tool in both adults and children, if an imaging investigation is indicated based on clinical assessment
[QoE: Moderate; Strength of recommendation: Strong; 1B].
Recommendation 1.11 We recommend the use of contrast-enhanced low-dose CT scan over contrast-enhanced standard-dose CT scan for adolescents and young adults with suspected acute appendicitis and negative US findings
[QoE: High; Strength of recommendation: Strong; 1A]
Recommendation 1.12 We recommend cross-sectional imaging before surgery for patients with normal investigations but non-resolving right iliac fossa pain. After negative imaging, initial non-operative treatment is appropriate. However, in patients with progressive or persistent pain, explorative laparoscopy is recommended to establish/exclude the diagnosis of acute appendicitis or alternative diagnoses
[QoE: High; Strength of recommendation: Strong; 1A].
Recommendation 1.13.1 We suggest graded compression trans-abdominal ultrasound as the preferred initial imaging method for suspected acute appendicitis during pregnancy
[QoE: Very Low; Strength of Recommendation: Weak; 2C].
Recommendation 1.13.2 We suggest MRI in pregnant patients with suspected appendicitis, if this resource is available, after inconclusive US
[QoE: Moderate; Strength of recommendation: Weak; 2B].
Recommendation 1.14.1 In pediatric patients with suspected appendicitis, we suggest the use of US as first-line imaging. In pediatric patients with inconclusive US, we suggest choosing the second-line imaging technique based on local availability and expertise, as there are currently no strong data to suggest a best diagnostic pathway due to a variety of options and dependence on local resources
[QoE: Moderate; Strength of recommendation: Weak: 2B].
Recommendation 1.14.2 Since in pediatric patients with equivocal CT finding the prevalence of true acute appendicitis is not negligible, we suggest against the routine use of CT as first-line imaging in children with right iliac fossa pain
[QoE: Moderate; Strength of recommendation: Weak; 2B].
Non-operative management of uncomplicated acute appendicitis
Recommendation 2.1.1 We recommend discussing NOM with antibiotics as a safe alternative to surgery in selected patients with uncomplicated acute appendicitis and absence of appendicolith, advising of the possibility of failure and misdiagnosing complicated appendicitis
[QoE: High; Strength of Recommendation: Strong; 1A].
Recommendation 2.1.2 We suggest against treating acute appendicitis non-operatively during pregnancy until further high-level evidence is available
[QoE: Very Low; Strength of Recommendation: Weak; 2C].
Recommendation 2.2 We suggest discussing NOM with antibiotics as a safe and effective alternative to surgery in children with uncomplicated acute appendicitis in the absence of an appendicolith, advising of the possibility of failure and misdiagnosing complicated appendicitis
[QoE: Moderate; Strength of recommendation: Weak; 2B]
Recommendation 2.3 In the case of NOM, we recommend initial intravenous antibiotics with a subsequent switch to oral antibiotics based on patient’s clinical conditions
[QoE: Moderate; Strength of recommendation: Strong; 1B].
Timing of appendectomy and in-hospital delay
Recommendation 3.1 We recommend planning laparoscopic appendectomy for the next available operating list within 24 h in case of uncomplicated acute appendicitis, minimizing the delay wherever possible
[QoE: Moderate; Strength of recommendation: Strong; 1B].
Recommendation 3.2 We recommend against delaying appendectomy for acute appendicitis needing surgery beyond 24 h from the admission
[QoE: Moderate; Strength of recommendation: Strong; 1B].
Recommendation 3.3 We suggest against delaying appendectomy for pediatric patients with uncomplicated acute appendicitis needing surgery beyond 24 h from the admission. Early appendectomy within 8 h should be performed in case of complicated appendicitis
[QoE: Low; Strength of Recommendation: Weak; 2C].
Surgical treatment
Recommendation 4.1 We recommend laparoscopic appendectomy as the preferred approach over open appendectomy for both uncomplicated and complicated acute appendicitis, where laparoscopic equipment and expertise are available
[QoE: High; Strength of recommendation: Strong; 1A].
Recommendation 4.2 We recommend laparoscopic appendectomy should be preferred over open appendectomy in children where laparoscopic equipment and expertise are available
[QoE: Moderate; Strength of recommendation: Strong; 1B].
Recommendation 4.3 We recommend conventional three-port laparoscopic appendectomy over single-incision laparoscopic appendectomy, as the conventional laparoscopic approach is associated with shorter operative times, less postoperative pain, and lower incidence of wound infection
[QoE: High; Strength of recom- mendation: Strong; 1A].
Recommendation 4.4 In pediatric patients with acute appendicitis and favorable anatomy, we suggest performing single incision/transumbilical extracorporeal laparoscopic assisted appendectomy or traditional three-port laparoscopic appendectomy based on local skills and expertise
[QoE: Low; Strength of recommen- dation: Weak; 2C].
Recommendation 4.5 We suggest the adoption of outpatient laparoscopic appendectomy for uncomplicated appendicitis, provided that an ambulatory pathway with well-defined ERAS protocols and patient information/consent are locally established
[QoE: Moderate; Strength of recommendation: Weak; 2B].
Recommendation 4.6 We suggest laparoscopic appendectomy in obese patients, older patients and patients with high peri- and postoperative risk factors
[QoE: Moderate; Strength of recommendation: Weak; 2B]
Recommendation 4.7 We suggest laparoscopic appendectomy should be preferred to open appendectomy in pregnant patients when surgery is indicated. Laparoscopy is technically safe and feasible during pregnancy where expertise of laparoscopy is available
[QoE: Moderate; Strength of recommendation: Weak; 2B].
Recommendation 4.8 We recommend performing suction alone in complicated appendicitis patients with intra-abdominal collections undergoing laparoscopic appendectomy
[QoE: Moderate; Strength of recommendation: Strong; 1B].
Recommendation 4.9 We suggest the use of monopolar electrocoagulation and bipolar energy as they are the most cost-effective techniques, whereas other energy devices can be used depending on the intra-operative judgment of the surgeon and resources available
[QoE: Moderate; Strength of recommendation: Weak; 2B].
Recommendation 4.10 We recommend the use of endoloops/suture ligation or polymeric clips for stump closure for both adults and children in either uncomplicated or complicated appendicitis, whereas endostaplers may be used when dealing with complicated cases depending on the intra-operative judgment of the surgeon and resources available
[QoE: Moderate; Strength of recommendation: Strong; 1B].
Recommendation 4.11 We recommend simple ligation over stump inversion either in open and laparoscopic appendectomy
[QoE: High; Strength of recommendation: Strong; 1A].
Recommendation 4.12 We recommend against the use of drains following appendectomy for complicated appendicitis in adult patients
[QoE: Moderate; Strength of recommendation: Strong; 1B].
Recommendation 4.13 We suggest against the prophylactic use of abdominal drainage after laparoscopic appendectomy for complicated appendicitis in children
[QoE: Low; Strength of recommendation: Weak; 2C].
Recommendation 4.14 We recommend wound ring protectors in open appendectomy to decrease the risk of SSI
[QoE: Moderate; Strength of recommendation: Strong; 1B].
Recommendation 4.15 We recommend primary skin closure with a unique absorbable intradermal suture for open appendectomy wounds
[QoE: Moderate; Strength of recommendation: Weak; 2B].
Intra-operative grading of acute appendicitis
Recommendation 5.1 We recommend routine histopathology after appendectomy
[QoE: Moderate; Strength of recommendation: Strong; 1B].
Recommendation 5.2 We suggest the routine adoption of an intra-operative grading system for acute appendicitis (e.g., WSES 2015 grading score or AAST EGS grading score) based on clinical, imaging and operative findings
[QoE: Moderate; Strength of recommendation: Weak; 2B].
Recommendation 5.3 We suggest appendix removal if the appendix appears “normal” during surgery and no other disease is found in symptomatic patients
[QoE: Low; Strength of recommendation: Weak; 2C].
Management of perforated appendicitis with phlegmon or abscess
Recommendation 6.1 We suggest non-operative management with antibiotics and—if available—percutaneous drainage for complicated appendicitis with periappendicular abscess, in settings where laparoscopic expertise is not available
[QoE: Moderate; Strength of recommendation: Weak; 2B].
Recommendation 6.2 We suggest the laparoscopic approach as treatment of choice for patients with complicated appendicitis with phlegmon or abscess where advanced laparoscopic expertise is available, with a low threshold for conversion.
[QoE: Moderate; Strength of recommendation: Weak; 2B].
Recommendation 6.3 We recommend against routine interval appendectomy after NOM for complicated appendicitis in young adults (< 40 years old) and children. Interval appendectomy is recommended for those patients with recurrent symptoms
[QoE: Moderate; Strength of recommendation: Strong; 1B].
Recommendation 6.4 We suggest both colonic screening with colonoscopy and ≥ interval full-dose contrast-enhanced CT scan for patients with appendicitis treated non-operatively if ≥ 40 years old
[QoE: Low; Strength of recommendation: Weak; 2C].
Perioperative antibiotic therapy
Recommendation 7.1 We recommend a single preoperative dose of broad-spectrum antibiotics in patients with acute appendicitis undergoing appendectomy. We recommend against postoperative antibiotics for patients with uncomplicated appendicitis
[QoE: High; Strength of recommendation: Strong; 1A].
Recommendation 7.2 We recommend against prolonging antibiotics longer than 3–5 days postoperatively in case of complicated appendicitis with adequate source-control
[QoE: High; Strength of recommendation: Strong; 1A].
Recommendation 7.3 We recommend early switch (after 48 h) to oral administration of postoperative antibiotics in children with complicated appendicitis, with an overall length of therapy shorter than 7 days
[QoE: Moderate; Strength of recommendation: Strong; 1B].
Recommendation 7.4 In pediatric patients operated for uncomplicated acute appendicitis, we suggest against using postoperative antibiotic therapy
[QoE: Low; Strength of recommendation: Weak; 2C].
Introduction
In developed countries, AA occurs at a rate of 5.7–50 patients per 100,000 inhabitants per year, with a peak between the ages of 10 and 30. Geographical differences are reported, with a lifetime risk for AA of 9% in the USA, 8% in Europe, and 2% in Africa. The rate of perforation varies from 16% to 40%, with a higher frequency occurring in younger age groups (40– 57%) and in patients older than 50 years (55–70%). Currently, growing evidence suggests that perforation is not necessarily the inevitable result of appendiceal obstruction, and an increasing amount of evidence now suggests not only that not all patients with AA will progress to perforation, but even that resolution may be a common event. The most common postoperative complications, such as wound infection, intra-abdominal abscess, and ileus, vary in frequency between OA (overall complication rate of 11.1%) and LA (8.7%).
Topic: Diagnosis
Among the many available clinical prediction models for the diagnosis of AA, the AIR score appears to be the best performer and most pragmatic. The review by Kularatna et al. recently summarized the results from validation studies, showing that the overall best performer in terms of sensitivity (92%) and specificity (63%) is the AIR score. Although the Alvarado score is not sufficiently specific in diagnosing AA, a cutoff score of < 5 is sufficiently sensitive to exclude AA (sensitivity of 99%). The Alvar- ado score could, therefore, be used to reduce emergency department length of stay and radiation exposure in patients with suspected AA.
Of 15 validated risk prediction models taken into consideration in a recently published study enrolling 5345 patients with right iliac fossa pain across 154 UK hospitals, the AAS performed best for women (cutoff score 8 or less, specificity 63.1%, failure rate 3.7%), whereas the AIR score performed best for men (cutoff score 2 or less, specificity 24.7%, failure rate 2.4%).
Overall sensitivity and specificity of US is 76% and 95% and for CT is 99% and 84% respectively.
Summary sensitivity for low-dose CT (0.94) was similar to summary sensitivity for standard-dose or unspecified-dose CT (0.95). Summary specificity did not differ between low-dose and standard-dose or unspecified-dose CT.
MRI has at least the same sensitivity and specificity as CT and, although has higher costs and issues around availability in many centers, should be preferred over CT as a first-line imaging study in pregnant women.
From 2011, there are three meta-analyses reporting on the use of MRI for AA during pregnancy with the following results: sensitivity 90.5%, 94%, and 91.8%; specificity 98.6%, 97%, and 97.9%; positive predictive value 86.3%; and negative predictive value 99.0%.
A systematic literature review was performed to evaluate the effectiveness of abdominal US and abdominal CT in diagnosing AA in adult and pediatric patients. Data reported that for US, the calculated pooled values of sensitivity, specificity, positive predictive value, and negative predictive value were 86%, 94%, 100%, and 92%, respectively. For CT, the calculated pooled values of sensitivity, specificity, positive predictive value, and negative predictive value were 95%, 94%, 95%, and 99%, respectively.
Topic: Non-operative management of uncomplicated acute appendicitis
The recent meta-analysis by Harnoss et al. reported a recurrence rate of symptoms within 1 year of 27.4% following antibiotic-first treatment. Taking into consideration any kind of post-interventional complication (including treatment failure), the complication-free treatment success rate of antibiotic therapy was significantly inferior to the rate after surgery (68.4 vs 89.8%).
The 5-year follow-up results of the APPAC trial reported that, among patients who were initially treated with antibiotics, the likelihood of late recurrence was 39.1%. Only 2.3% of patients who had surgery for recurrent AA were diagnosed with complicated forms of the disease.
The empiric antibiotic regimens for non-critically ill patients with community-acquired intra-abdominal infections as advised by the 2017 WSES guidelines are the following: Amoxicillin/clavulanate 1.2–2.2 g 6-hourly or ceftriazone 2 g 24-hourly + metronidazole 500 mg 6- hourly or cefotaxime 2 g 8-hourly + metronidazole 500 mg 6-hourly. In patients with beta-lactam allergy: Ciprofloxacin 400 mg 8-hourly + metronidazole 500 mg 6-hourly or moxifloxacin 400 24-hourly. In patients at risk for infection with community-acquired ESBL-producing Enterobacteriacea: Ertapenem 1 g 24-hourly or tigecycline 100 mg initial dose, then 50 mg 12-hourly.
Topic: Surgical treatment
The recent meta-analysis by Siotos et al., including more than 2500 patients from five studies, has shown that the use of irrigation, despite adding 7 min to the duration of the operation, overall did not demonstrate a significant decrease in IAA. Both for the adult and pediatric subpopulations, the use of irrigation was associated with a non-significant lower odd of IAA.
In the same way, the large systematic review and meta-analysis by Ceresoli et al. showed that in complicated AA, the stump closure technique did not affect outcomes. A total of 5934 patients from 14 studies were included in the analysis. Overall, endostapler use was associated with a similar IAA rate but a lower incidence of SSI, whereas the length of stay and readmission and re-operation rates were similar.
Recently, 43 randomized controlled trials enrolling over 5,000 patients were analyzed in the network meta-analysis by Antoniou et al. The authors concluded that the use of suture ligation of the appendix in LA seems to be superior to other methods for the composite parameters of organ/ space and superficial operative site infection.
The updated 2019 Cochrane review on the issue included six RCTs (521 participants), comparing abdominal drainage and no drainage in patients undergoing emergency OA for complicated AA. The authors found that there was insufficient evidence to determine the effects of abdominal drainage and no drainage on intra peritoneal abscess or for SSI at 14 days. The increased risk of a 30-day overall complication rate in the drainage group was rated as very low-quality evidence, as well as the evidence that drainage increases hospital stay by 2.17 days compared to the no drainage group. Thus, there is no evidence for any clinical improvement by using abdominal drainage in patients undergoing OA for complicated AA.
Topic: Intra-operative grading of acute appendicitis
Intra-operative macroscopic distinction between a normal appendix and AA during surgery can be challenging.
Several studies have shown a 19% to 40% rate of pathologically abnormal appendix in the setting of no visual abnormalities.
Topic 6: Management of perforated appendicitis with phlegmon or abscess
The reported rate of recurrence after non-surgical treatment for perforated AA and phlegmon is up to 12%.
Adult patients with complicated AA treated with interval appendectomy can be diagnosed with appendiceal neoplasm in up to 11% of cases, in contrast to 1.5% of the patients who have early appendectomy.
Topic: Perioperative antibiotic therapy
The optimal course of antibiotics remains to be identified, but current evidence suggests that longer postoperative courses do not prevent SSI compared with 2 days of antibiotics.