Moren AM, Biffl WL, Ball CG, de Moya M, Brasel KJ, Brown CVR, et al. Blunt pancreatic trauma: A Western Trauma Association critical decisions algorithm. J Trauma Acute Care Surg. 2023;94:455–60. https://journals.lww.com/10.1097/TA.0000000000003794
Explanation
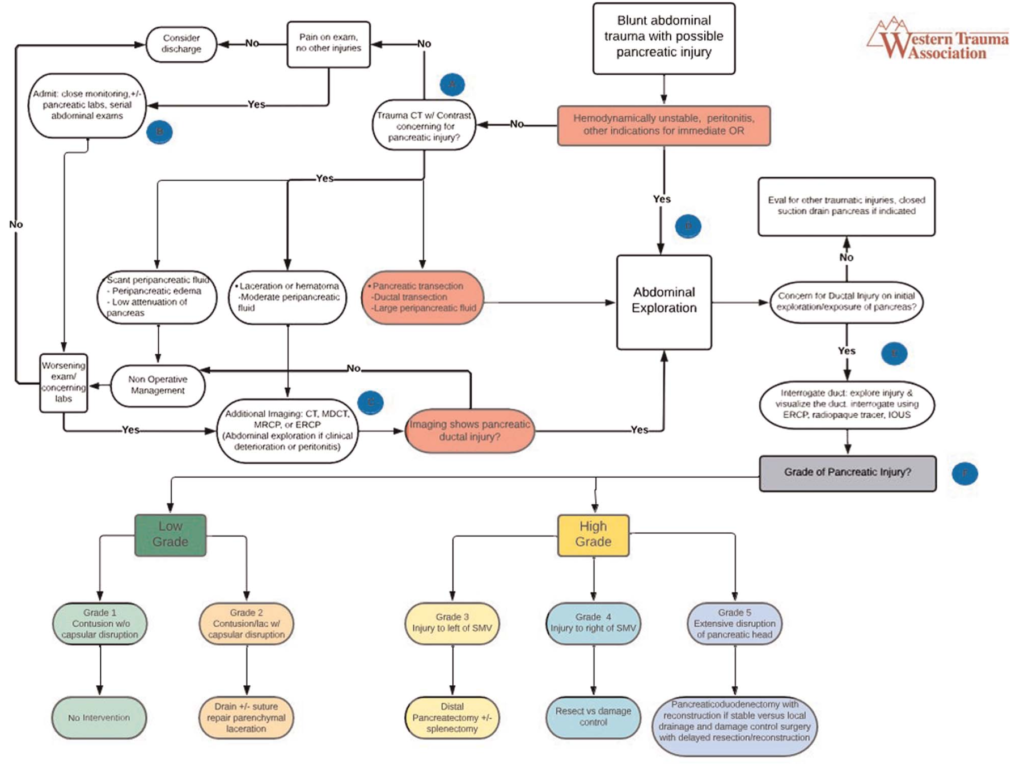
Among patients with BPI, approximately 20% have indications for immediate laparotomy and will have an intraoperative diagnosis.
A
The sensitivities for detecting BPI are variable, ranging from 47% to 79%, with specificities between 90% and 95%. Although not available at all facilities, multidetector CT scanners, which provide 64 thin-slice imaging cuts, have been shown to improve the specificity of diagnosis of pancreatic duct injury (PDI) to as high as 91% to 100%. Increased risk of PDI is associated with lacerations involving greater than 50% of the width of the pan- creas, pancreatic contusions, and active hemorrhage on CT. The findings of transection of the pancreas or main pancreatic duct (MPD), or a large amount of peripancreatic fluid, should lead to operative exploration given the likelihood of PDI and the need for surgical management.
B
Laboratories: Both amylase and lipase have proven nonspecific for BPI; however, if one enzyme were to be used, lipase has been shown to be slightly better at indicating pancreatic injury. One prospective study found elevated enzyme levels to predict BPI when imaging was nondiagnostic within 6 hours after injury. Other studies have shown that serum pancreatic enzyme values are not specific enough to diagnose or exclude BPI, although elevated levels should heighten concern for occult injury. Buechter et al. reported that enzymes collected on admission and through day 7 were nonspecific. Although elevated pancreatic enzymes are not reliable in either isolated or serial settings to diagnose pancreatic trauma, they have been seen to correlate with BPI >6 hours after initial injury. These elevations seen hours after injury may be useful in diagnosing late or missed injury and should prompt additional imaging.
C
Additional imaging: The diagnosis of BPI requires high clinical suspicion. Therefore, if the initial CT scan appears normal but objective findings of an elevated lipase or amylase >6 hours from time of injury, and/or subjectively the patient has worsening abdominal pain, concern for BPI should prompt additional imaging. As many as 40% of CT scans in patients with pancreatic injury are initially interpreted as normal. Repeat CT with IV contrast is recommended if clinical concern remains. In the patient with nonspecific findings as previously mentioned, and a clinical concern for injury, pancreatography is recommended to direct further management.
Magnetic resonance cholangiopancreatography should still be considered first-line imaging for PDI, but findings should be interpreted cautiously if they do not match clinical suspicion.
Endoscopic retrograde cholangiopancreatography (ERCP) is one of the most sensitive tools to detect ductal injury. Advantages of ERCP include the ability to evaluate main duct versus branch duct injuries and to perform therapeutic sphincterotomy or pancreatic duct stenting. Although stenting has been discussed as an adjunct to nonoperative management (NOM), a recent WTA multicenter trial found that this is rare and that two thirds of stents were placed to manage PRCs. Enthusiasm for primary stenting is further tempered by the findings of Kim et al. and Bhasin et al., who reported an association of early pancreatic stenting with pancreatic duct strictures, local and systemic sepsis, and potential worsening of the injury.
E
Low grade: Although PDI is associated with a significant increase in PRCs, there can still be significant morbidity associated with low-grade injuries. Based on the recent multicenter WTA trial, the lowest rate of PRCs is seen after NOM (4%), which is recommended in those patients who have no other indication for laparotomy. For low-grade injuries diagnosed intraoperatively, drain placement is recommended only if there is pancreatic capsule disruption. This is based on an incidence of PRCs of 26% after drainage of blunt low-grade injuries. If there is evidence of capsular disruption, drainage is recommended to control the leakage. However, resection of low-grade injuries should be avoided, as the occurrence of PRCs (42%) is significantly higher after resection compared with other management strategies.
Grade III: Distal pancreatectomy has long been recommended for grade III injuries. Biffl et al. noted that there was no difference in PRCs between patients treated with resection (41%) compared with those treated with drainage (29%), raising the possibility that drainage may be a noninferior option. Until this is studied prospectively, distal pancreatectomy remains the recommendation for grade III injuries.
F
Pancreatic related complications: Complications from pancreatic injuries carry significant morbidity and mortality, including fluid collections, leaks, hemorrhage, fistulae, and chronic sequelae of pseudocysts. For patients with drains, amylase levels should be followed on days 1 and 3 after placement. Those with drain amylase less than that of serum can be removed. Persistent pancreatic leak should prompt further imaging and possible intervention.