Weinberg JA, Peck KA, Ley EJ, Brown C V., Moore EE, Sperry JL, et al. Evaluation and management of bowel and mesenteric injuries after blunt trauma: A Western Trauma Association critical decisions algorithm. J Trauma Acute Care Surg. 2021;91:903–8
Introduction
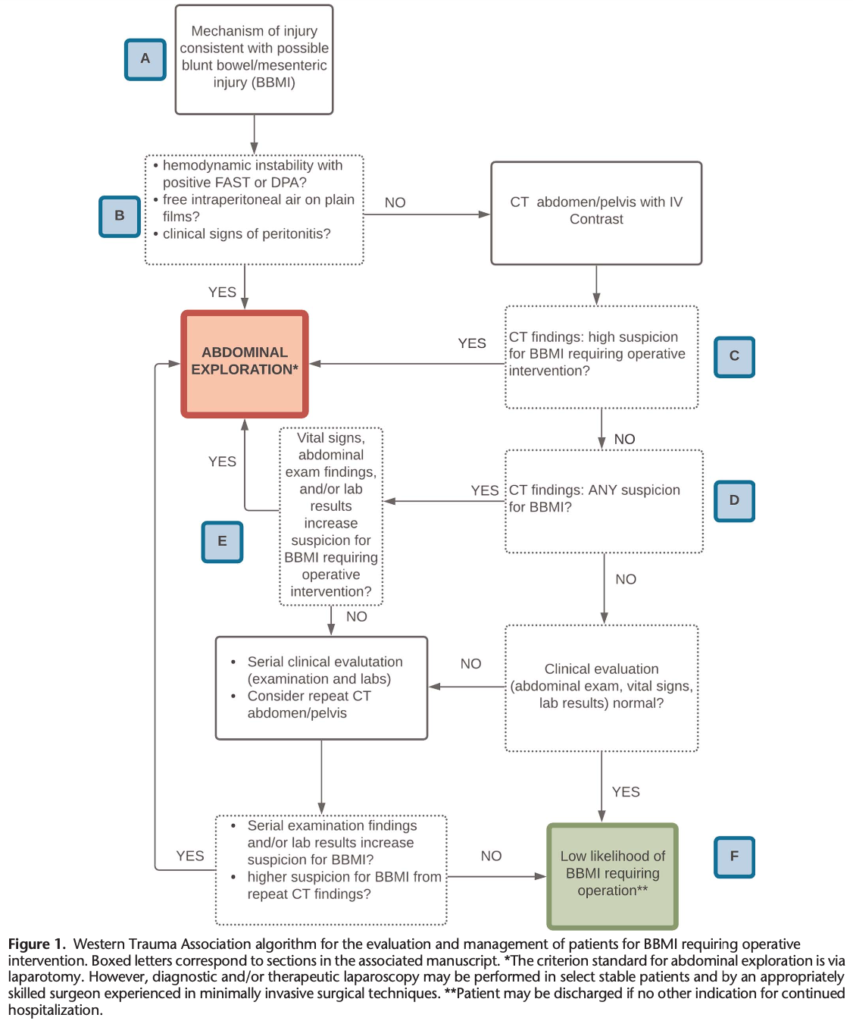
Unrecognized significant BBMI is the most frequent cause for delayed intervention after blunt abdominal trauma, and a diagnostic delay of 5 to 8 hours has a negative impact on survival. Nonetheless, 45% to 70% of patients with evidence for BBMI on initial CT imaging will not require surgical repair, and nontherapeutic laparotomy exposes patients to risk for both early and late complications including atelectasis, wound complications, adhesive bowel obstruction, and incisional hernia.
A:
Typical scenarios would include direct blows to the abdomen (physical assault, seatbelt compression), high-speed vehicular collisions, fall from significant height, pedestrian or cyclist struck by vehicle at high speed, and impact of restraints causing sudden increase in intra-abdominal pressure.
C:
There are three pathognomonic CT findings or “hard signs” for BBMI: bowel wall discontinuity (which may be seen with or without oral contrast), extraluminal air (with the exception of pneumo-peritoneum as a result of pneumothorax as described in Section B8), and vascular blush or extravasation in the mesentery. These three findings warrant operative management.
These “soft signs” include free fluid (particularly in the absence of solid organ injury), focal bowel wall thickening, nonenhancing bowel, and mesenteric stranding. The presence of multiple soft signs should signal to the surgeon that significant BBMI is likely and operative intervention is warranted.
In the absence of solid organ injury, free fluid is more worrisome but may nonetheless be relatively benign: phys- iologic in women or a result of self-limited bleeding from an inconsequential rent in the retroperitoneum or mesentery that has collected in the peritoneal cavity. In female patients, free pelvic fluid isolated to the pouch of Douglas that is low in density and does not extend more superiorly than the S3 body may be considered “physiologic.” Nonetheless, any amount of free fluid associated with any of the other soft signs as described previously suggests significant BBMI, and operative intervention is warranted. A moderate to large volume of free fluid with no other soft signs present (either in the absence of solid organ injury or relative to what would be expected from solid organ injury in a stable patient) is highly suspicious for BBMI and also warrants operative intervention. In addition to bowel injury, the fluid may be indicative of intraperitoneal bladder rupture. A caveat to this directive would be suspicion that the free fluid is not blood, urine, and/or succus but rather ascites related to underlying cirrhosis (a known history of cirrhosis, morphologic characteristics of a cirrhotic liver on CT, and/or low-density simple fluid would support this suspicion and could be confirmed by needle aspiration of the free fluid). Nonetheless, erring toward the side of operative versus intervention versus observation is recommended, given the known mortality risk associated with delay.
D:
Such findings would include isolated soft signs, such as mesenteric stranding or small volume free fluid, often described in radiology reports as “trace.” Other findings that warrant suspicion for BBMI include traumatic abdominal wall hernia and seatbelt-related stranding and/or hematoma of the abdominal wall. For patients with any of these findings on CT imaging, BBMI cannot be ruled out, and consideration of the patient’s clinical picture in context with the CT findings is warranted.
E:
Should the CT scan reveal any suspicion for BBMI, clinical judgment is necessary with respect to choosing operative intervention versus serial clinical examination with or without repeat imaging. Systemic/constitutional findings such as tachycardia or fever increase the likelihood of significant BBMI, as does abdominal ecchymosis (i.e., the “seat belt sign”), and tenderness and/or distention in the setting of an abnormal CT scan. Leukocytosis and/or acidosis can also suggest significant BBMI.
The duration of observation necessary to exclude significant BBMI remains unclear; at least 24 hours is recommended. Repeat CT scan approximately 24 hours following admission may be used to evaluate for changes in appearance of fluid and/or stranding or for new findings such as extraluminal air. This may be particularly useful for patients with an unreliable physical examination secondary to associated brain injury or other neurologic compromise.
F:
A patient may have a significant mesenteric tear that is not evident on initial imaging but results in insidious bowel ischemia and late presentation of segmental bowel necrosis, which can occur 3 to 7 days following injury.
Patients with an abnormal initial CT who are observed for at least 24 hours without clinical worsening, especially with a repeat CT that demonstrates stability or improvement of the initial CT findings, are also unlikely to have underlying significant BBMI. The decision to continue surveillance beyond this time must be individualized according to the patient’s CT findings (minimal vs. more extensive), examination reliability (awake, tolerating diet vs. obtunded from extra-abdominal injuries, substance abuse, etc.), and overall injury burden.