Tesoriero, Ronald, Raul Coimbra, Walter L. Biffl, Clay Cothren Burlew, Chasen A. Croft, Charles Fox, Jennifer L. Hartwell, u. a. „Adult Emergency Resuscitative Thoracotomy: A Western Trauma Association Clinical Decisions Algorithm“. Journal of Trauma and Acute Care Surgery 97, Nr. 6 (Dezember 2024): 961–68. https://doi.org/10.1097/TA.0000000000004462.
Explanations
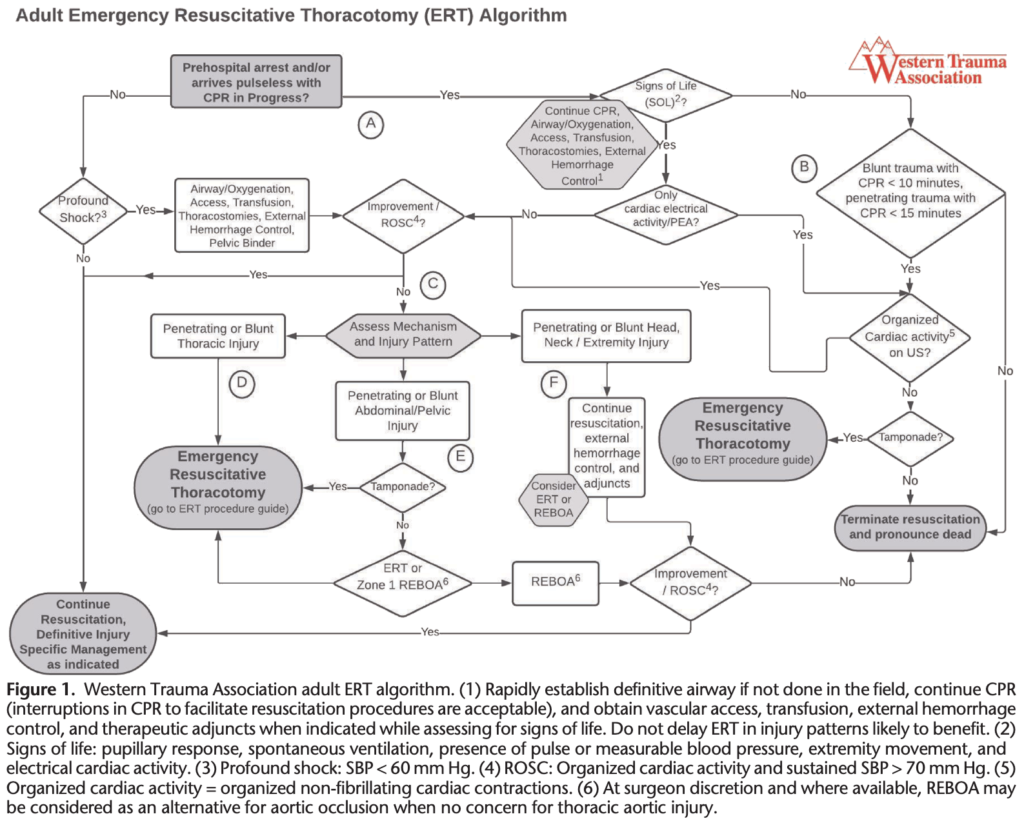
While chest compressions have not been clearly demonstrated to improve outcomes in posttraumatic arrest, they may be helpful in patients who have a source of cardiac arrest other than hemorrhage or whose cause of arrest is suspected to be medical. However, in animal models of arrest due to hemorrhagic shock, closed chest compressions (CCC) have failed to demonstrate an improvement in arterial pressure and have been associated with a lower likelihood of ROSC than volume resuscitation alone. Although continuation of CCC in traumatic arrest is reasonable, their performance should not impede or delay establishment of intravenous access and volume resuscitation, procedures used to address reversible causes of traumatic cardiac arrest, ERT, or AO. Mechanical compression devices impede access to the chest and if placed by prehospital providers should be removed on arrival to facilitate evaluation and resuscitation procedures.
Emergency resuscitative thoracotomy and AO are not indicated in those with profound shock or cardiac arrest who respond to initial resuscitation and adjunctive treatment with ROSC, defined as a perfusing organized cardiac rhythm and a sustained systolic blood pressure of >70 mm Hg. Resuscitation should continue aiming for rapid movement to definitive hemorrhage control and injury specific management.
Survival for blunt trauma patients presenting without SOL ranges from 0% to 0.7%, while it ranges from 1.6% to 8.3% in penetrating trauma. The likelihood of neurologically intact survival is higher with penetrating thoracic injury compared with penetrating extrathoracic or blunt injury and is greatest with cardiac stab wounds. For those presenting without SOL, there seems to be a time signature that predicts futility. A 2011 multicenter study demonstrated survivors of blunt traumatic arrest with up to 9 minutes of cardiopulmonary resuscitation (CPR) and after penetrating trauma with up to 15 minutes of CPR. However, the only survivors in the extremes of these times had evidence of pericardial tamponade. Others have not been able to show survival in blunt trauma when SOL are absent, and the Eastern Association for the Surgery of Trauma guidelines have conditionally recommended not performing ERT for blunt trauma patients without SOL
When SOL other than CEA are present, a rapid evaluation of response to resuscitation and assessment of mechanism/injury pattern as indicated in section C should occur. In the absence of SOL, blunt trauma patients presenting with greater than 10 minutes and penetrating truncal trauma patients presenting with greater than 15 minutes of prehospital CPR should have resuscitation terminated and be pronounced dead. Those presenting within the described time parameters are considered for ERT. FAST should search for the presence of organized cardiac wall motion or tamponade in patients without SOL and when CEA is the only SOL. Patients with organized wall motion should be rapidly assessed for response to initial resuscitation and mechanism/injury pattern with treatment selection as indicated in section C. Patients with tamponade and asystole should undergo ERT. If cardiac windows are difficult to interpret, consideration for ERT should be made carefully based on mechanism of injury, duration of CPR, and presence of CEA. Patients with absent cardiac wall motion and without tamponade on adequate FAST evaluation should have resuscitation terminated and be pronounced dead.
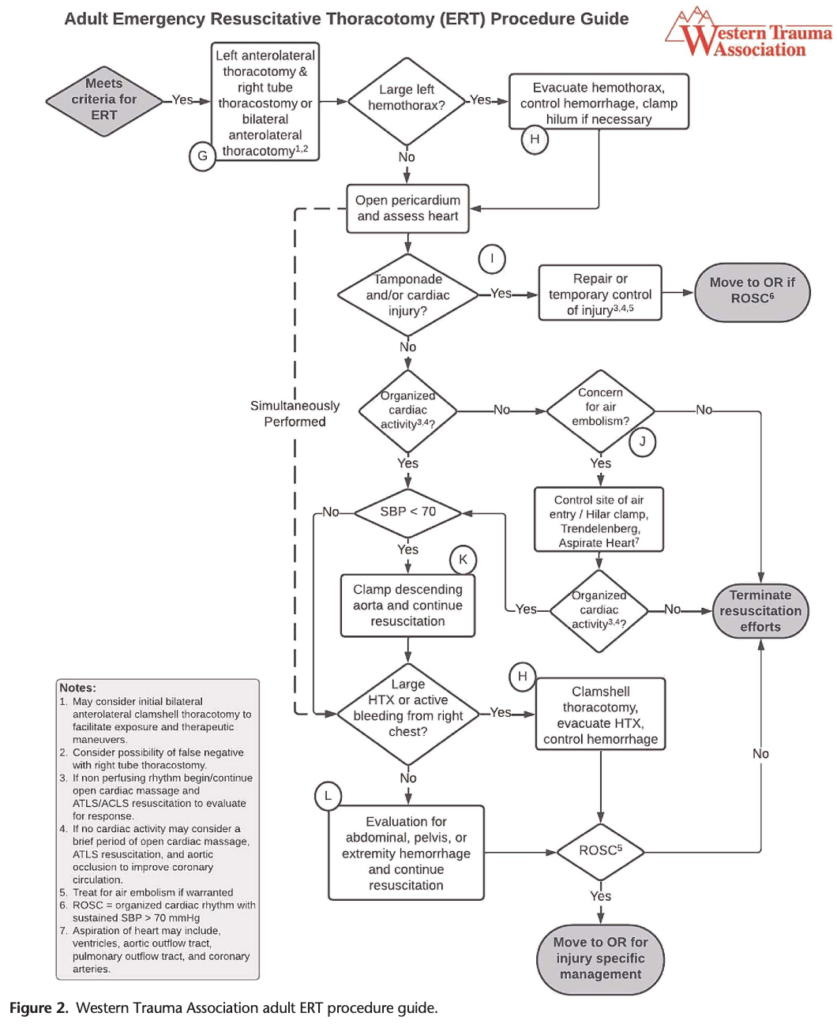
Patients meeting the criteria for ERT who present with penetrating thoracic trauma, penetrating truncal trauma with a trajectory concerning for thoracic injury, or obvious blunt thoracic injury should undergo ERT without delay, as they are more likely to have injuries that will benefit from direct control and management through thoracic exploration in addition to OCC and descending thoracic AO.
Patients with penetrating or blunt abdominal/pelvic trauma who present with profound shock or traumatic cardiac arrest should be considered for early femoral arterial access in centers that practice REBOA. A rapid cardiac FAST examination should be performed, and those who have evidence of tamponade should undergo ERT. If tamponade is absent and the injury pattern is not concerning for concomitant thoracic trajectory or blunt aortic injury, REBOA may be considered as an alternative to ERT where training and local expertise exist. For patients selected for REBOA, early transition to ERT should be considered if rapid femoral access is difficult to obtain. Patients who achieve ROSC after Zone 1 AO by REBOA should be rapidly transported to a site where definitive hemorrhage control and injury specific management can occur without delays for diagnostic testing. Where REBOA is unavailable, injury pattern suggests benefit, or when preferred by the surgeon, the patient should undergo ERT. Those who achieve adequate AO and fail to achieve a perfusing organized cardiac rhythm with a systolic blood pressure of >70 mm Hg should have resuscitation terminated and be pronounced dead.
Patients with isolated penetrating or severe blunt head injury or penetrating or blunt injury to the neck or extremities who fail to respond to resuscitation and hemorrhage control should have resuscitation terminated and be pronounced dead.
Conclusion
Emergency resuscitative thoracotomy should be considered in those with profound shock who fail to respond to resuscitation, those in arrest with SOL other than electrical cardiac activity, for patients with CEA as the only SOL if organized cardiac activity is seen on ultrasound, and in those without SOL presenting within described time parameters with cardiac activity on ultrasound or asystole in the presence of tamponade. Alternative methods of AO and cardiac compressions may be considered in select patients unlikely to benefit from direct thoracic exploration and hemorrhage control.