Explanations
A Cochrane Review examined early versus delayed laparoscopic CCY for uncomplicated biliary colic. Early CCY was performed within 24 hours, while the mean waiting time to delayed CCY was 4.2 months. The early group had significantly shorter operating time (by 14.8 minutes) and hospital stay (by 1.25 days) and fewer serious adverse events (0% vs. 23%). Conversion to open CCY occurred in 0% in the early group and 17% in the delayed group (p = 0.07).
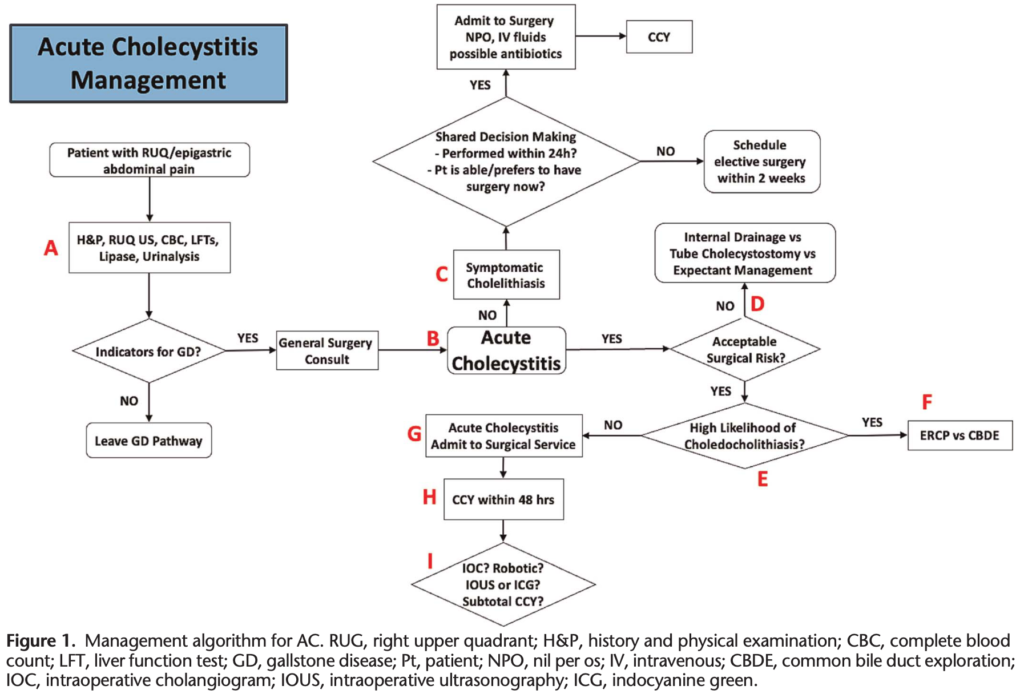
If the patient cannot be accommodated for prompt CCY or would prefer doing it at a more convenient time, arrangements should be made to have them undergo elective surgery within the ensuing 2 weeks to decrease the risk of repeated ED visits.
The CHOCOLATE trial, comparing PT-GBD versus laparoscopic CCY in high-risk patients, was stopped after a planned interim analysis because of a higher number of major complications (65% vs. 12%) and recurrent biliary disease (53% vs. 5%) in the PT-GDB group with no mortality difference. However, the study enrolled patients based on Apache II scores of 7 to 14, which, in the opinion of many of the current authors, would not represent particularly high surgical risk. A 2022 systematic review and metaanalysis of six studies (n = 8,960) comparing PT-GBD with laparoscopic CCY for acute calculous cholecystitis in high-risk surgical patients reported that PT-GBD was associated with significantly higher risks of mortality, morbidity, readmission rate, and hospitalization length. Following PT-GBD, interval CCY is generally recommended if the patient’s risk profile improves. If the patient is still not an acceptable surgical risk for CCY, transition to EUS-GBD or ETP-GBD is a potential option. While some authors report a high degree of success of interval laparoscopic CCY, others have reported longer operative times and increased rates of conversion, surgical site infection, bowel injury, and 1-year mortality associated with interval CCY compared with acute CCY. The common practice of routine surveillance cholangiography prior to CCY has been called into question by Loftus et al. based on increased resource utilization and delays to drain removal and CCY.
The DRAC 1 randomized trial compared EUS-GBD with PT-GBD in very high-risk surgical patients (80 years or older, American Society of Anesthesiologists Physical Status Classification System score ≥III, Age-adjusted Charlson Comorbidity Index >5, or Karnofsky score <50) and found that EUS-GBD significantly reduced 30-day and 1-year adverse events, reinterventions, unplanned readmission, and recurrent cholecystitis (2.6% vs. 20%, p = 0.029).
A systematic review with network meta-analysis compared the three methods of gallbladder drainage in high-risk patients with AC and found that the three modalities have their respective advantages and disadvantages. For example, EUS-GBD was associated with the lowest risk of recurrent cholecystitis, PT-GBD had the highest risk of reintervention and unplanned readmissions, and the lowest mortality rates were seen after ETP-GBD. Selecting the most appropriate technique will depend on available expertise and anatomic considerations. To date, data on the use of EUSGBD have almost exclusively been derived from older patients deemed to be at prohibitive operative risk, who never undergo CCY. Its use in younger patients or those likely to later be candidates for CCY should be undertaken only after careful consideration given the lack of data on long-term patency and increased technical difficulty of CCY after lumen-apposing stent placement.
The ASGE guidelines recommend prompt endoscopic retrograde cholangiopancreatography (ERCP) in patients with high-risk predictors, given the positive predictive value of 85%. Given the availability and efficacy of ERCP, it has become firmly inculcated in clinical practice. Consequently, the performance of common bile duct exploration has been on a downward trend for many years, from 40% of admissions for choledocholithiasis in 1998 to less than 10% in 2013. However, there is a high rate (nearly 45%) of discordance from ASGE guidelines in practice. For example, the insistence on “confirmatory” magnetic resonance cholangiopancreatography before ERCP delays definitive management and is of questionable benefit when one factors in the suboptimal sensitivity of this screening modality. In recent years, the advantages of single-stage management have been recognized. Intraoperative ERCP combined with CCY saves resources and shortens hospital LOS. There has also been a resurgence of interest in laparoscopic common bile duct exploration, and several authors have described its safety and efficacy.
In a population-based analysis, de Mestral et al. identified adults with a first emergency admission for uncomplicated AC. Among 25,397 patients, 41% did not undergo CCY during the first admission. The probability of a gallstone-related event by 6 weeks, 12 weeks, and 1 year after discharge was 14%, 19%, and 29%, respectively. Moreover, 30% of these events were for pancreatitis or biliary tract obstruction. Patients with AC are best served on a surgical service, with reduced length of stay, resource utilization, and costs.
Zafar et al. found that laparoscopic CCY performed within 2 days of presentation of AC was associated with fewer complications, lower mortality, and lower costs. A recent retrospective cohort study of National Surgical Quality Improvement Program data found that late operation (>48 hours) for AC was associated with higher mortality. Among elderly (older than 65 years) patients with comorbidities, CCY within 24 hours of admission was associated with shorter hospital and postoperative stays without an increase in morbidity, mortality, or conversion from laparoscopic to open surgery. It is important to recognize that older patients are at higher risk for gangrenous cholecystitis, of which US findings may be absent or minimal and delay in surgical consultation is common. Centers with the resources to perform CCY at night and on the weekends should do so without concerns of increased complications.
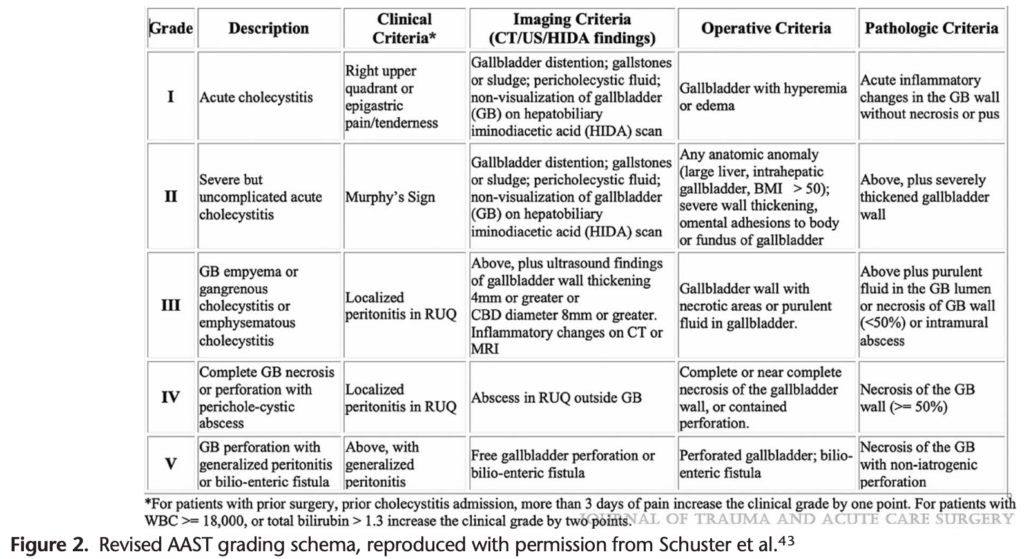
The revised American Association for the Surgery of Trauma (AAST) grading scale for AC (Fig. 2) is one such tool, with higher grades predicting conversion from laparoscopic to open procedure, use of surgical bail-out procedures, bile leak, and major complications.