de’Angelis N, Schena CA, Marchegiani F, Reitano E, De Simone B, Wong GYM, et al. 2023 WSES guidelines for the prevention, detection, and management of iatrogenic urinary tract injuries (IUTIs) during emergency digestive surgery. World J Emerg Surg 2023;18:45. doi:10.1186/s13017-023-00513-8.
Introduction
The reported incidence of iatrogenic ureteral injury during elective abdominal surgery ranges between 0 and 1.5%; this increases in emergency settings.
Based on a recent nationwide survey of Swiss general surgeons, formal identification of the left ureter during sigmoid colectomy or rectal surgery was considered mandatory by 83.7% of participants, while only 31.7% considered the identification of the right ureter mandatory during right colectomy.
Statements
Statement 1.1
Complex diverticular disease, T4-stage colorectal cancer, history of previous abdominal or pelvic surgery, malnutrition, and obesity are risk factors of increased operative complexity and predictors of IUTI. In case of patient- and disease-related risk factors for IUTI, we recommend that the surgical team considers preventive interventions, discussing the risks and benefits of these adjuncts with the patient.
Weak recommendation, low quality of evidence (GRADE 2C)
Strength of consensus: 98%
Statement 1.2
A specific preoperative imaging work-up to assess anatomical landmarks and consequential proper abdominal cavity access (e.g., trocar positioning or laparotomic incision) are effective and reliable strategies to prevent IUTI.
Weak recommendation, very low quality of evidence (GRADE 2D)
Strength of consensus: 90%
Statement 1.3
Ureteral stents should be considered as a valuable strategy for ureteral IUTI prevention and identification in selected, high-risk patients undergoing open and minimally invasive emergency digestive surgery. In selected, high-risk patients, lighted and fluorescent ureteral catheters should be considered as a useful tool during minimally invasive surgery.
Weak recommendation, low quality of evidence (GRADE 2C)
Strength of consensus: 98%
Statement 1.4
Fluorescent dyes (intraureteral indocyanine green and intravenous methylene blue) may be considered as an adjunct for real-time ureteral identification and prevention of IUTI in selected patients undergoing minimally invasive emergency digestive surgery, where difficulties in localizing the ureters are expected.
Weak recommendation, low quality of evidence (GRADE 2C)
Strength of consensus: 94%
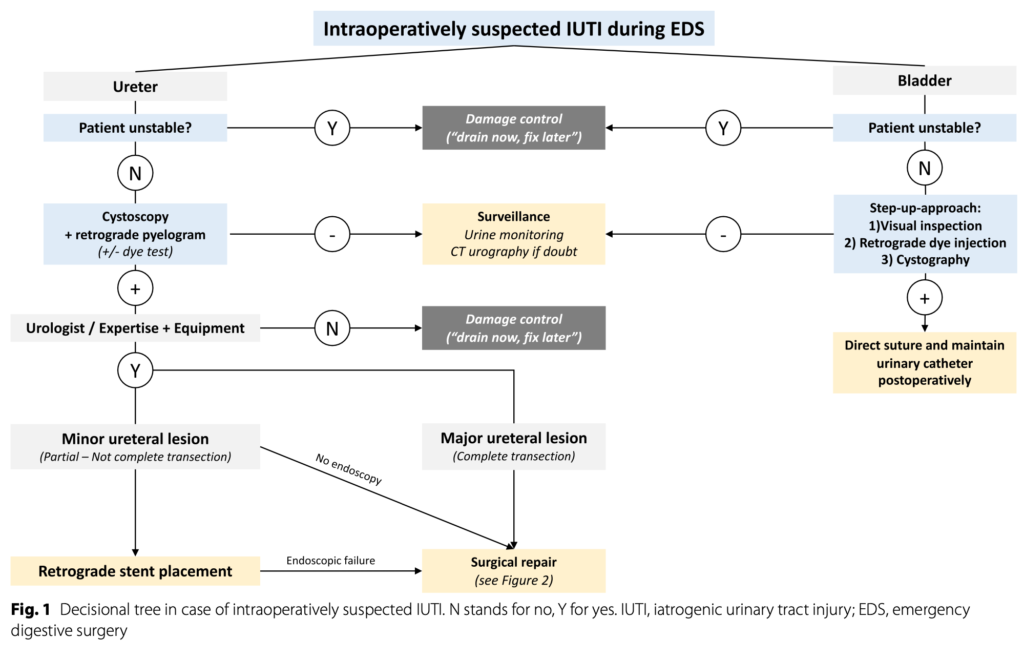
Statement 2.1
Prompt intraoperative diagnosis and staging of IUTI, according to the hemodynamic status of the patient, are essential to assure the best management and reduce postoperative morbidity and mortality. A high level of IUTI suspicion should be maintained in high-risk patients.
Weak recommendation, low quality of evidence (GRADE 2C)
Strength of consensus: 94%
Statement 2.2
The gold standard of intraoperative IUTI detection is the diagnostic cystoscopy with retrograde pyelogram. This requires the patient to be hemodynamically stable and properly positioned, and it is also limited by the availability of dedicated equipment (e.g., mobile C-arm machine, operating room with radiation shielded walls and doors, C-arm compatible operating table) and urological expertise. Alternative diagnostic tools, such as intraoperative dye tests (e.g., indigo carmine intravenous injection), direct ureteral inspection or retrograde ureteral catheterization, can be utilized to aid in detecting IUTI when the previous conditions are not satisfied.
Weak recommendation, low quality of evidence (GRADE 2C)
Strength of consensus: 96%
Statement 2.3
In cases of confirmed IUTIs, intraoperative repair is the preferred option depending on the patient’s status and availability of urologic expertise (see Statements 2.5, 3.5, 3.6 and 3.7).
Weak recommendation, low quality of evidence (GRADE 2C)
Strength of consensus: 94%
Statement 2.4
In case of IUTI occurring during minimally invasive procedures, laparoscopic/robotic repair can be performed if sufficient surgical expertise is available. In case of insufficient surgical expertise, a “drain now, fix later” approach can be adopted, or a conversion to an open surgery can be considered to repair the IUTI.
Weak recommendation, low quality of evidence (GRADE 2C)
Strength of consensus: 96%
Statement 2.5
Intraperitoneal bladder injuries should be directly repaired with a 2-layer adsorbable suture. Urinary catheter should be positioned and maintained for at least 7 days with a negative retrograde cystography performed before its removal. Ureteral stenting or nephrostomy tubes placement is an option in case of wide bladder injuries or injuries close to the ureteral orifices.
Strong recommendation, moderate quality evidence (GRADE 1B)
Strength of consensus: 98%
Statement 3.1
Serum and peritoneal fluid biochemical markers may be considered as useful diagnostic tools in case of suspected IUTI if CT urography is not available and in low-resource conditions. IUTI are often associated with increased serum inflammation markers (e.g., C-RP), decreased renal function, increased peritoneal fluid creatinine and urea, or altered ratio between serum and peritoneal fluid creatinine.
Strong recommendation, moderate quality evidence (GRADE 1C)
Strength of consensus: 90%
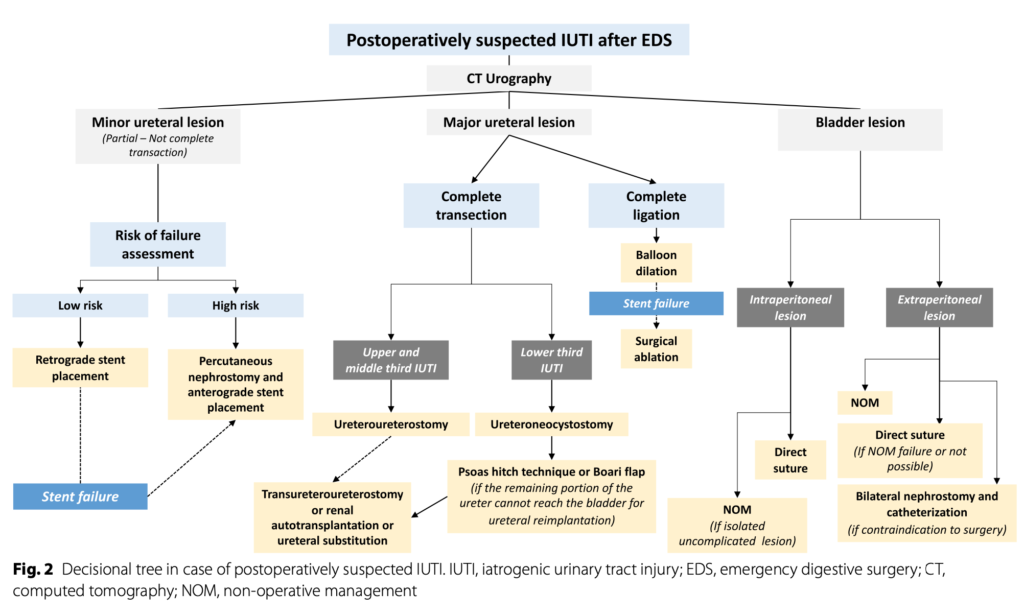
Statement 3.2
CT urography with both nephrographic and excretory phases represents the gold standard diagnostic exam for the postoperative diagnosis of IUTI.
Strong recommendation, moderate quality evidence (GRADE 1B)
Strength of consensus: 98%
Statement 3.3
Ureteral IUTI diagnosed postoperatively should be treated as soon as possible to avoid complications and sepsis.
Strong recommendation, moderate quality evidence (GRADE 1B)
Strength of consensus: 100%
Statement 3.4
In partial ureteral transection, minimally invasive techniques (endoscopic or radiological), such as retrograde or anterograde stent positioning, should be attempted as a first-line treatment.
Strong recommendation, low quality of evidence (GRADE 1C)
Strength of consensus: 98%
Statement 3.5
Ureteroureterostomy is the preferred surgical techniques for the treatment of upper and middle third IUTI of the ureter. The anastomosis should be stented and, if possible, covered with peritoneum or other tissue.
Strong recommendation, low quality evidence (GRADE 1C)
Strength of consensus: 96%
Statement 3.6
IUTI of the lower third of the ureter requires direct reimplantation. If this is not possible, more complex procedures, such as psoas hitch technique or Boari flap are indicated. An ureteral stent should be positioned.
Strong recommendation, low quality evidence (GRADE 1C)
Strength of consensus: 98%
Statement 3.7
Major intraperitoneal bladder injuries diagnosed postoperatively should be treated by surgical repair as reported above (Statement 2.5), while postoperative non-operative management based on urinary catheter placement could be considered in case of isolated uncomplicated (no signs of peritonitis or ileus) intraperitoneal and extraperitoneal injuries. Urinary catheter should be maintained for at least 7 days for intraperitoneal bladder injuries and at least 5 days for extraperitoneal bladder injuries, with a negative retrograde cystography performed before its removal.
Strong recommendation, low quality evidence (GRADE 1C)
Strength of consensus: 92%
Statement 4.1
In the case of IUTI diagnosed intraoperatively, antimicrobial treatment should not be administered.
Weak recommendation, very low quality evidence (GRADE 2D).
Strength of consensus: 81%
Statement 4.2
Empirical broad-spectrum antibiotic therapy against Enterobacteriaceae and Enterococci in association with adequate and timely source control is recommended in case of IUTI with signs of infection, sepsis, or septic shock to start as soon as possible. The dose and timing of antimicrobial administration should be adapted to the patient’s weight, renal clearance, and liver function. Antibiotic treatment must be adapted to the results of hemocultures and microbiological cultures.
Strong recommendation, high quality evidence (GRADE 1B)
Strength of consensus: 100%
Statement 4.3
Empirical antifungal therapy is not recommended for IUTI.
Strong recommendation, moderate quality evidence (GRADE 1C)
Strength of consensus: 98%
Statement 4.4
In cases with adequate source control, short-course antibiotic therapy (3–5 days) with early re-evaluation according to the clinical course and laboratory parameters is recommended, also in critically ill patients.
Strong recommendation, high quality evidence (GRADE 1A)
Strength of consensus: 100%
Statement 4.5
In patients with an indwelling urinary catheter or ureteral stents who develop symptomatic urinary tract infections following IUTI, empiric antibiotic treatment should be initiated and continued until the causative microorganism is identified and its susceptibility to antibiotics is determined.
Weak recommendation, moderate quality of evidence (GRADE 2B)
Strength of consensus: 98%